
An end to cervical cancer is possible
And some countries are already on track to do so.

We all have those moments in life where something clicks. A few years ago, I had mine when I realised that many cancers are caused by infections.
Before then, I had what I’d guess is the common understanding of how cancers form and spread. The cells in our body are continually growing, dividing, repairing and dying. Cancers start when mutations escape the usual process of repair or die, forming clusters of abnormal cells. These then divide and replicate, forming a tumour and invading nearby tissue.
Most of these mutations are random, so developing cancer is often down to bad luck. And then there are risk factors and lifestyle choices that increase the odds of getting various cancers. We all know the common ones: smoking, obesity, skin damage.
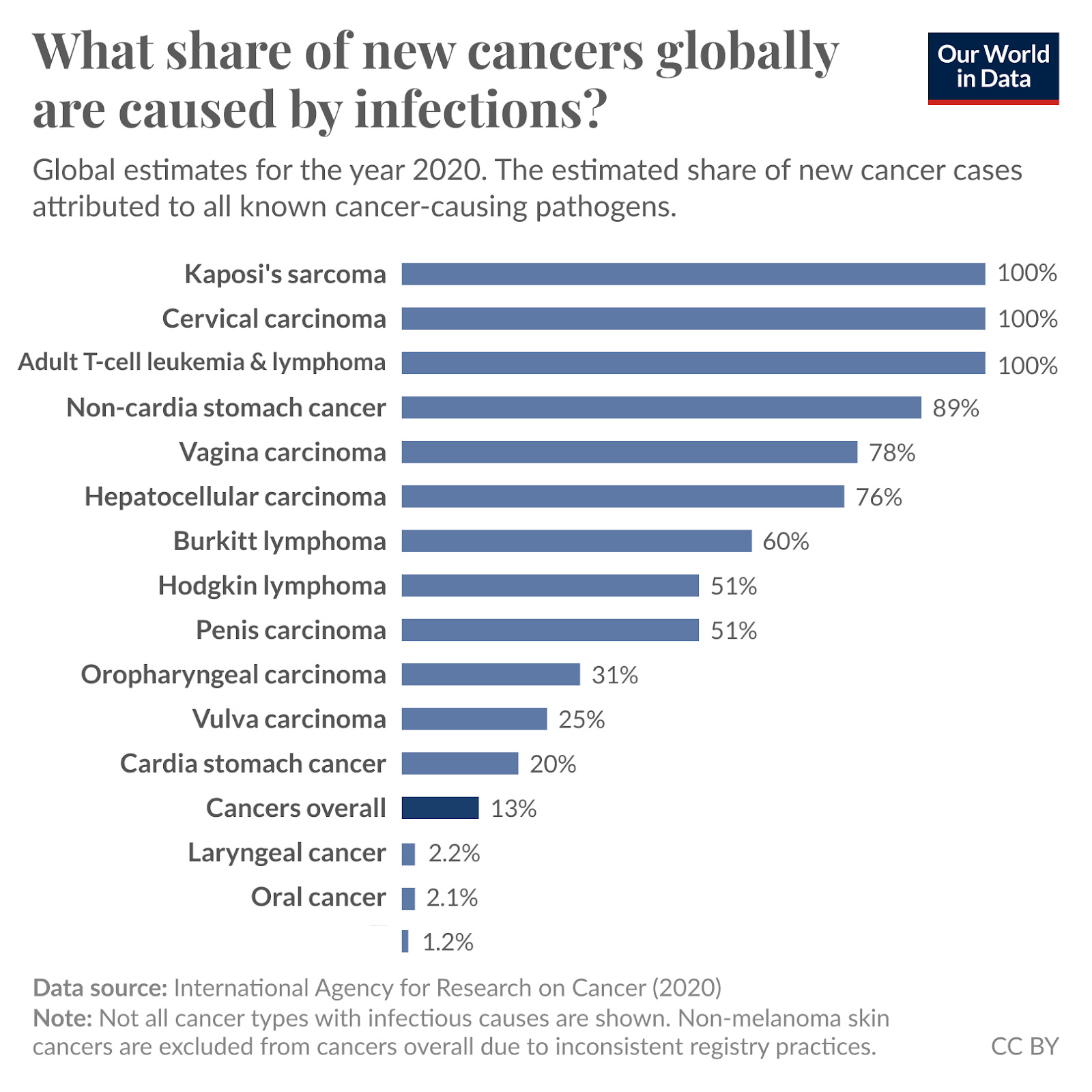
While I knew that certain viruses increase the risk of some cancers: human papillomavirus (HPV) for cervical cancer or hepatitis B and C for liver cancer, I underestimated how strong that link was. I also hadn’t quite internalised that many other cancers are caused by infections. Around 13% of cancers are, and for some types, infections are the largest cause.
This finally clicked for me a few years ago when talking to my former colleague, Saloni Dattani (who is an expert on all things health, and I’ve learned a lot from). You should follow her Substack, and the publication she co-founded, Works in Progress.
Many cancers are caused by infections, and we often know how to prevent them
The fact that many cancers are caused by infections is good news: humans have a decent track record of finding ways to beat infections. At least, we have a better idea of how to do that than just stopping random, unlucky cell mutations.
The most dramatic example of progress is stomach cancer. Most cases are caused by infection from Helicobacter pylori, which causes long-term damage and inflammation in the stomach and can eventually lead to cancer.
Improvements in hygiene and food safety standards have reduced the prevalence of H pylori across many countries, leading to a dramatic fall in stomach cancer death rates in recent decades.1
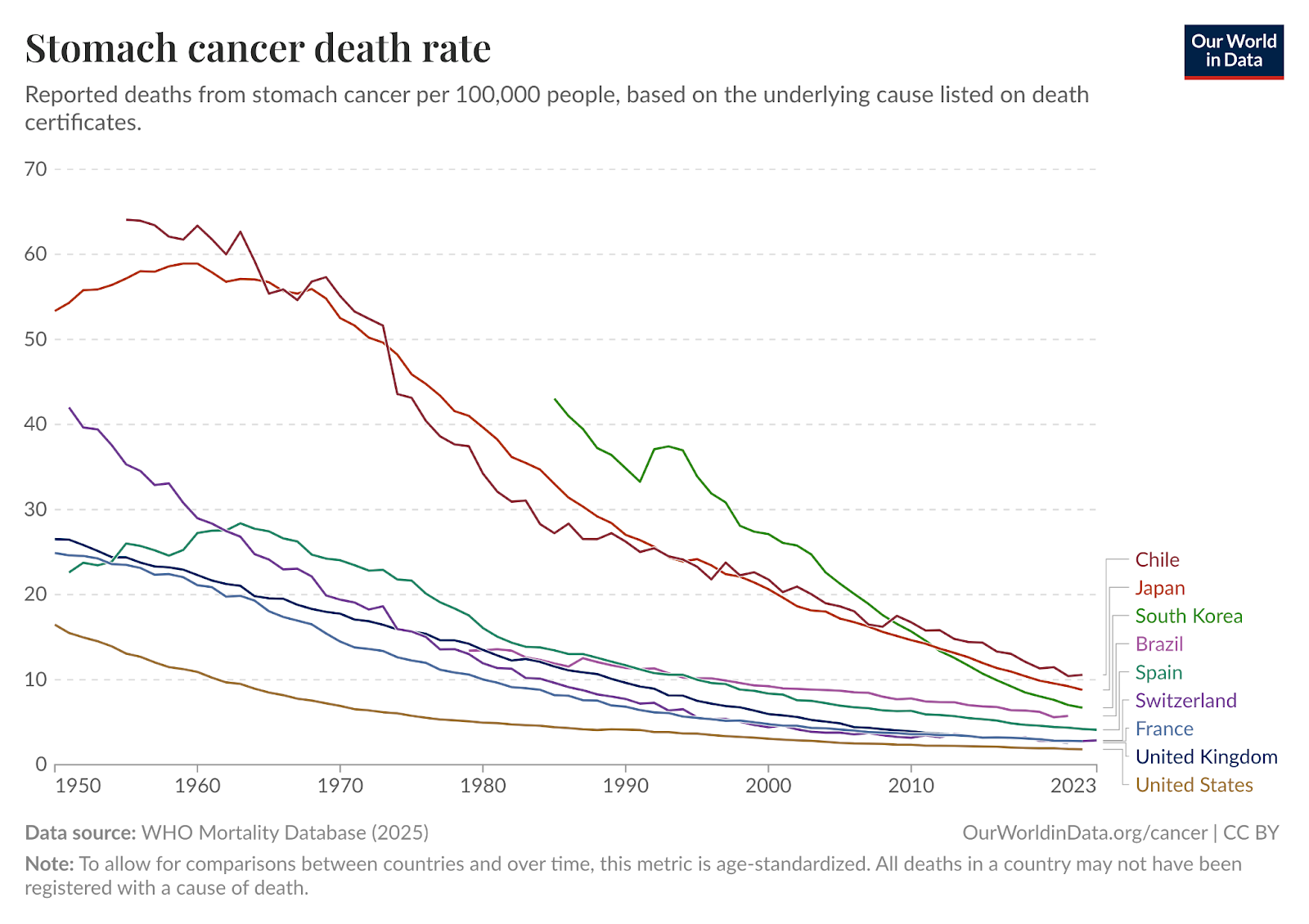
Globally, stomach cancer death rates have fallen by 60%. In some countries, the change has been even more dramatic. In Japan, stomach cancer was once the largest cancer killer, but death rates have fallen by more than 70%, and that’s no longer the case.
This decline in stomach cancer is not that well-known. The fact that it was caused by an infection is key to our success in tackling it. That is also true for cervical cancer, which we can and are making progress on.
The HPV vaccine offers extremely high protection against cervical cancer
I was among the first cohort of schoolgirls in Scotland to get the HPV vaccine. Class by class, we were marched down to join a queue to get “a jab that protected against cancer”.
I don’t think I quite internalised that this single vaccine could essentially stop me from getting an extremely common type of cancer later in life. Perhaps this was also because the vaccine’s effectiveness in large populations was not as well established as it is now. “This will reduce the risk of cervical cancer” is how it was framed, but by how much was underappreciated.
Nearly all cases of cervical cancer are caused by the human papillomavirus (HPV) infection.2 Many types of HPV are spread through sexual contact. An effective HPV vaccine, therefore, stops someone from becoming infected (and dramatically reduces the risk that they later develop cervical cancer as a result).
The fact that it typically spreads through sexual contact means that HPV vaccines need to be given to children before they reach puberty to be most effective. They’re typically recommended for girls aged 9 to 14 years. Vaccinating older adolescents also reduces the risk, but it is less effective than vaccinating at younger ages.
There is now a lot of evidence that these vaccines work. One thing that makes these studies difficult is that the risk of cervical cancer (like most cancers) tends to increase steeply with age. The cohorts of girls/women who were vaccinated before adolescence are still relatively young, so we can’t say from population data that girls vaccinated early are much less likely to develop cervical cancer in their 50s or 60s.
But we can say a lot about the prevalence of HPV infections and the development of cancerous cells among younger women.
Cochrane Reviews — often seen as the gold standard of research reviews — consistently find positive outcomes. A review of randomised control trials found that the HPV vaccine significantly reduces pre-cancerous outcomes.3 The same is true for reviews of population-level studies, which found that:
“There are now long‐term outcome data from different countries and from different study designs that consistently report a reduction in the development of high‐grade CIN and cervical cancer in females vaccinated against HPV in early adolescence. Data show that there is greater benefit to vaccinating younger adolescents prior to becoming sexually active.”4
This reduction in risk of developing cervical cancer was at least 80%.
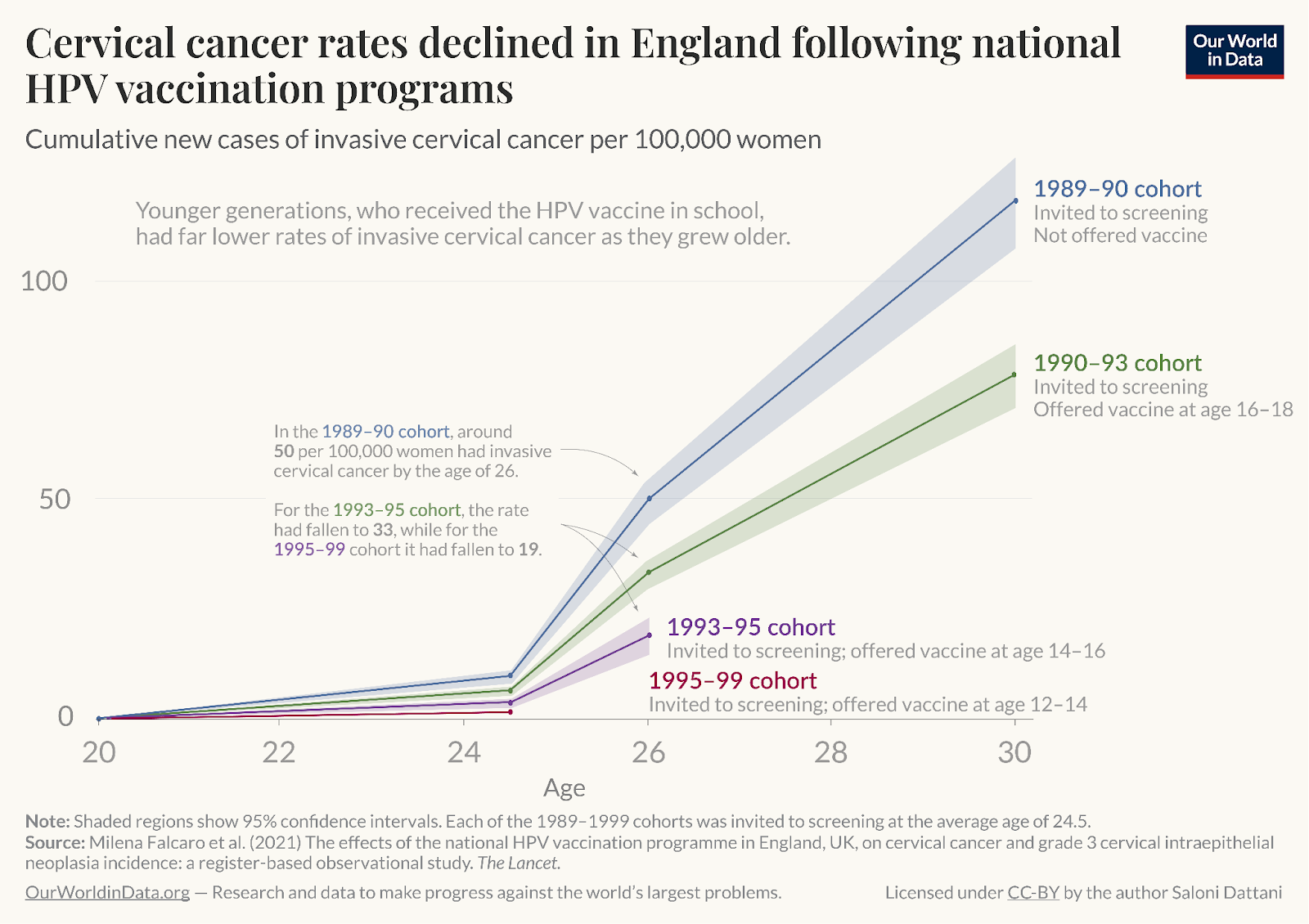
We can see this reduced risk clearly in studies from countries with national immunisation programs. Below is a chart that my former colleague, Saloni Dattani, made of cervical cancer rates among cohorts of young women in England.
On the x-axis, we have the women’s age. On the y-axis, the rates of new cervical cancer cases. As you can see from the blue and green lines (which represent different cohorts of women), cervical cancer risk increases with age. The blue line shows the new cases among women who were not offered the HPV vaccine. The green line shows those who were offered it at age 16 to 18. Girls who were vaccinated, even in their older teenage years, had a lower risk than those who were not vaccinated at all.
But you can then see the large reductions in risk among those vaccinated at younger ages. In purple are those vaccinated between the ages of 14 and 16. In red, those aged 12 to 14. These lines don’t extend as far along the x-axis, because these cohorts of women had not yet reached age 28 or 30 at the time of follow-up. But you can see that the line is consistently shallower and lowest among women vaccinated in their preteen years.
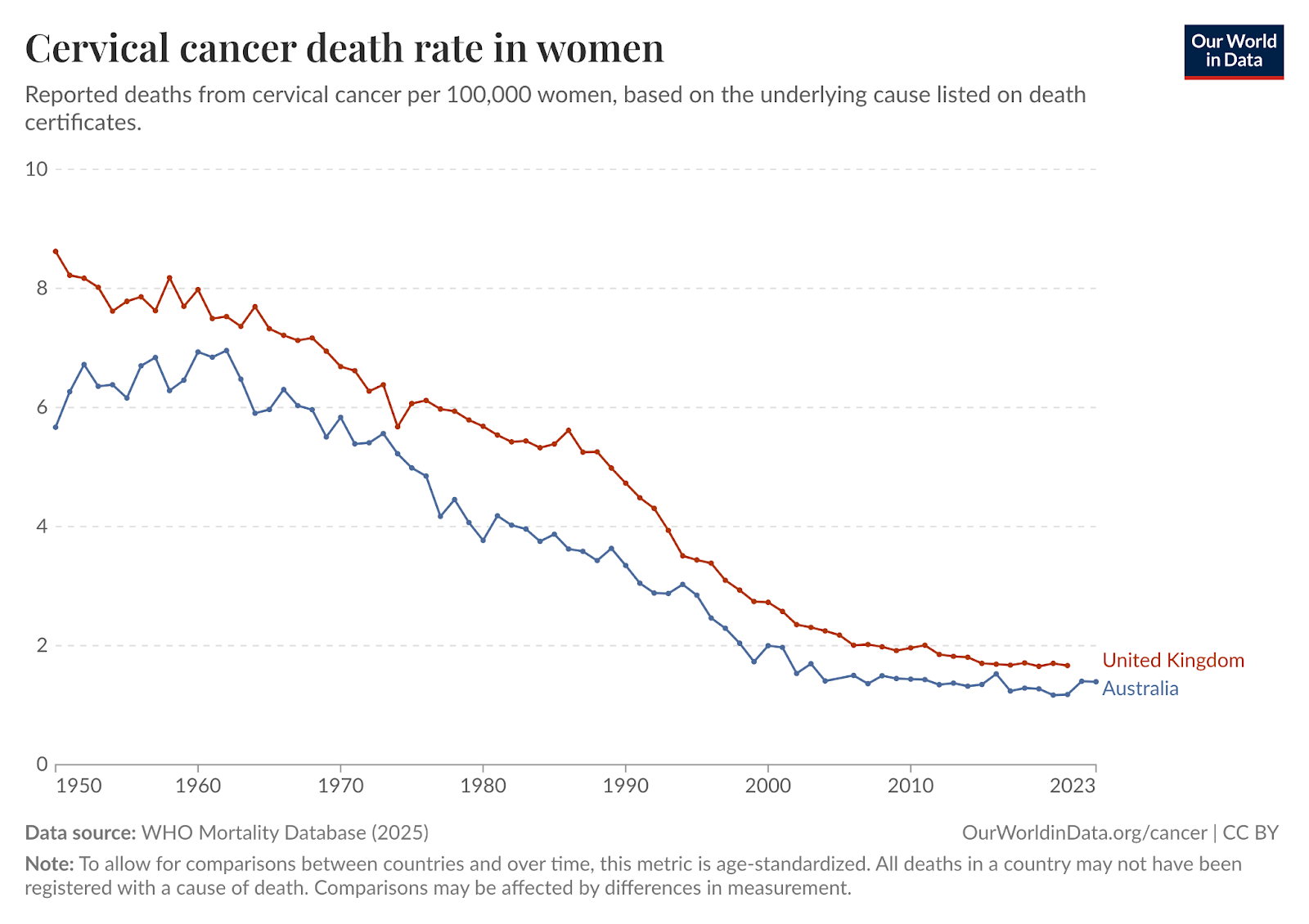
Similar evidence exists among populations of women in other countries with high vaccination rates. Australia is another stand-out example. It was the first country to launch a nationwide, publicly-funded vaccination program, and could be the first to eliminate cervical cancer completely.5
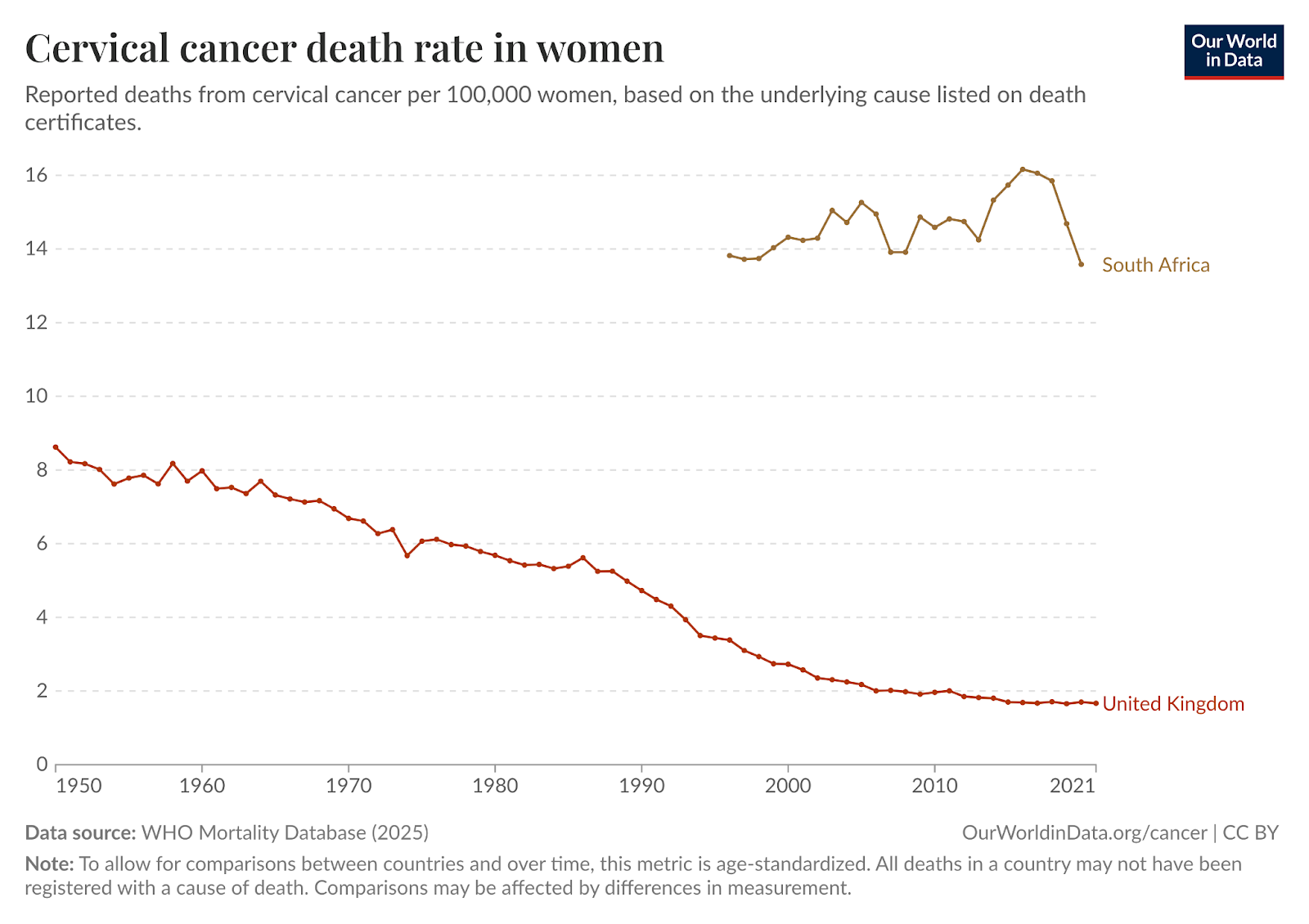
Combined with national smear test screening programs, both the UK and Australia have seen a dramatic reduction in death rates.
While most vaccine programs have been rolled out across high-income countries, there is huge potential for them in low- to middle-income countries, too.
A new study looking at the success of trials among young girls in South Africa is especially promising.6 It found a similar 80% reduction in HPV infections among girls who were vaccinated (achieving similar results with a two-dose program as those seen in three-dose programs in rich countries).
Importantly, this was also seen among girls who were living with HIV. This matters because having HIV can increase the risk of a HPV infection developing into cervical cancer. The high-burden of HIV is one of several reasons why death rates from cervical cancer are much higher in South Africa than in the UK.
Hundreds of thousands of women die from cervical cancer every year; we now know how to stop this for future generations
The fact that we have an incredibly effective vaccine against cervical cancer is huge.
Globally, there are between 600,000 and one million new cervical cancer cases each year, and around 370,000 women die from it.
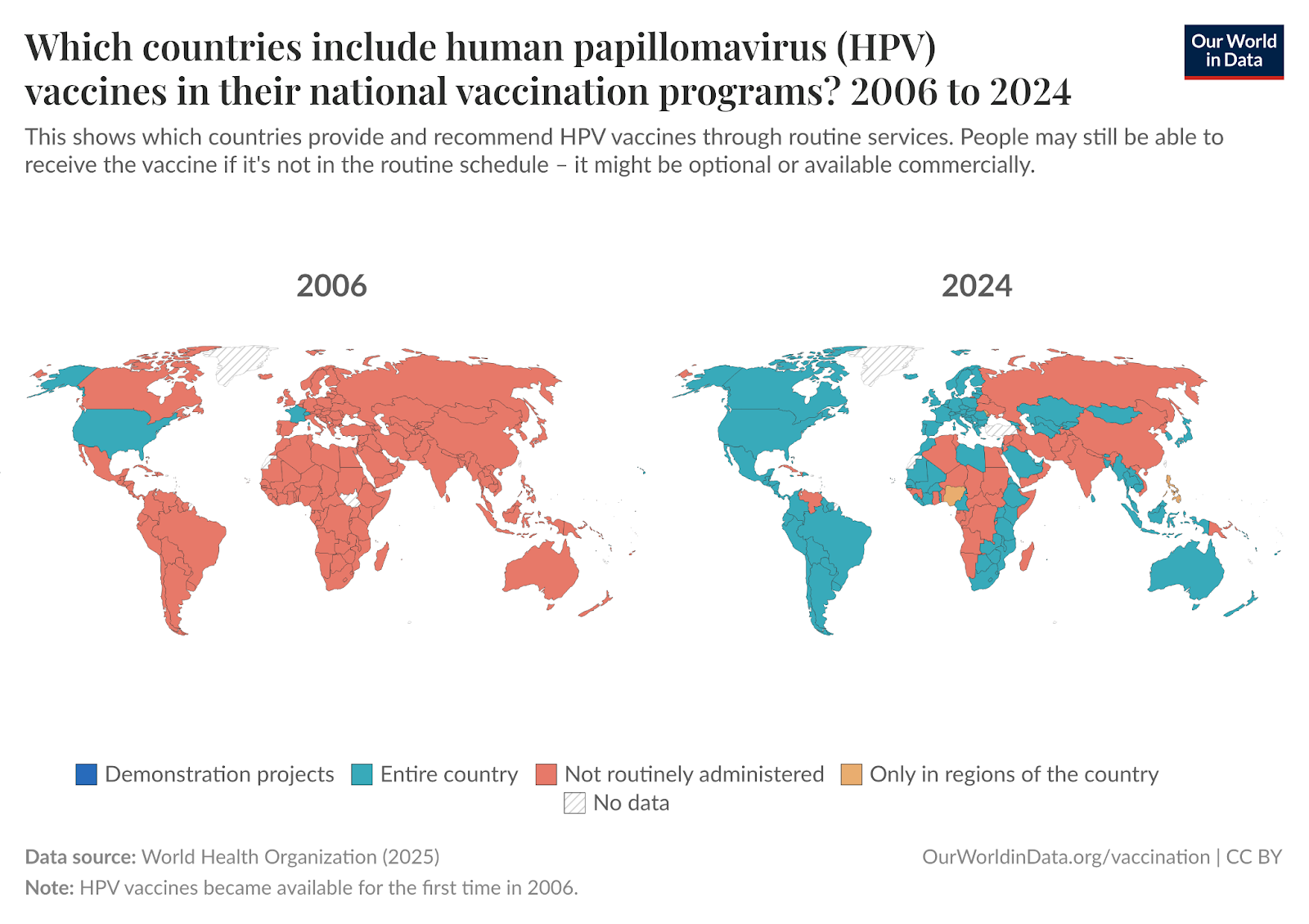
What’s crucial is the rollout of vaccination programs across the world. This is happening. In the two maps below, you can see the change in the number of countries with HPV vaccines in their national vaccination programs.
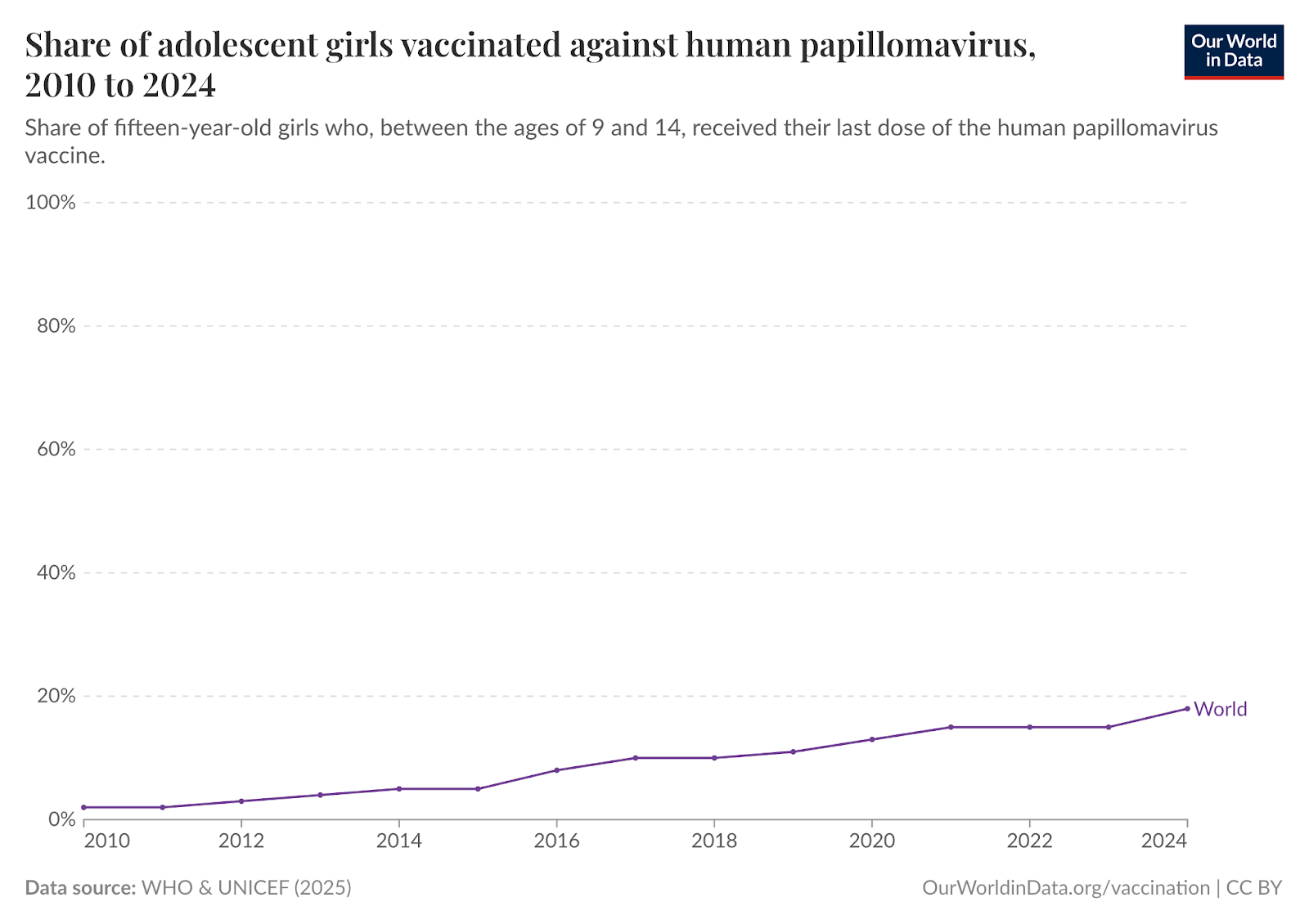
Nonetheless, only one-in-five fifteen-year-old girls today received the HPV vaccine schedule in their early adolescent years. There is still a long way to go.
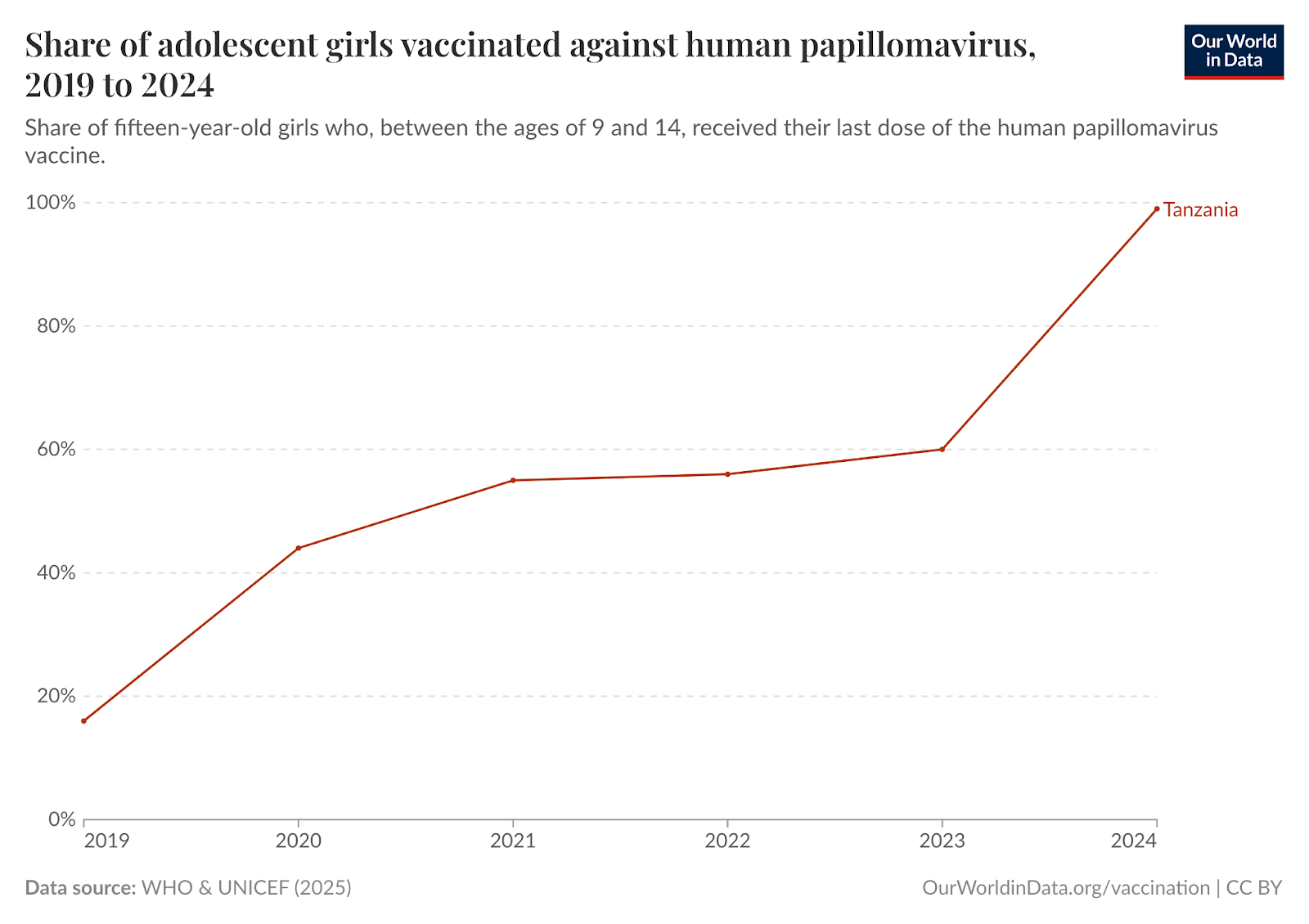
The exciting thing about these programs is that they can scale incredibly quickly, even in places with fairly limited health resources. Just look at Tanzania, another country with particularly high rates of cervical cancer due to HIV. Within a few years, it went from a minority of girls being vaccinated to almost universal coverage.
More efforts like this could see tens of millions of lives saved in the coming decades, and an end to one of the most common cancer types.
Improvements in early detection and treatment have also played a crucial role.
HPV can also cause a range of other cancers, including penile, anal, vaginal, and some head and neck cancers.
This is why many also recommend that boys get the vaccine too; they’re not vulnerable to cervical cancer, but it can reduce their risk of other ones.
Schiffman, M., Doorbar, J., Wentzensen, N., De Sanjosé, S., Fakhry, C., Monk, B. J., Stanley, M. A., & Franceschi, S. (2016). Carcinogenic human papillomavirus infection. Nature Reviews Disease Primers, 2(1), 16086.
Bergman, H., Henschke, N., Arevalo-Rodriguez, I., Buckley, B. S., Crosbie, E. J., Davies, J. C., ... & Morrison, J. (2025). Human papillomavirus (HPV) vaccination for the prevention of cervical cancer and other HPV‐related diseases: a network meta‐analysis. Cochrane Database of Systematic Reviews, (11).
Henschke, N., Bergman, H., Buckley, B. S., Crosbie, E. J., Dwan, K., Golder, S. P., ... & Morrison, J. (2025). Effects of human papillomavirus (HPV) vaccination programmes on community rates of HPV‐related disease and harms from vaccination. Cochrane Database of Systematic Reviews, (11).
Hall, M. T., Simms, K. T., Lew, J. B., Smith, M. A., Brotherton, J. M., Saville, M., ... & Canfell, K. (2019). The projected timeframe until cervical cancer elimination in Australia: a modelling study. The Lancet Public Health, 4(1), e19-e27.
Machalek, D. A., Nyemba, D. C., Travill, D., Petoumenos, K., Mbulawa, Z. Z., Naidoo, I., ... & Murray, G. L. (2026). Population impact of South Africa's human papillomavirus (HPV) vaccination programme on HPV prevalence in adolescent girls with and without HIV: a repeat cross-sectional study. The Lancet Global Health, 14(4), e570-e578.
I was going to comment that it's a shame India and China were both still red on that map, given their huge population and huge resources (relative to many poorer countries on that map who have rolled it out) - and I looked it up and they've both launched nationwide HPV programs very recently! China last November and India this March. Very good news.
Thank you for covering this. And! HPV vaccinations for boys means that they won’t suffer from HPV+ cancers either. I had oropharyngeal cancer, of which incidence amongst adults is quickly rising (now more common than cervical cancer in the UK https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(25)00181-1/fulltext ); there is no risk that my son will.